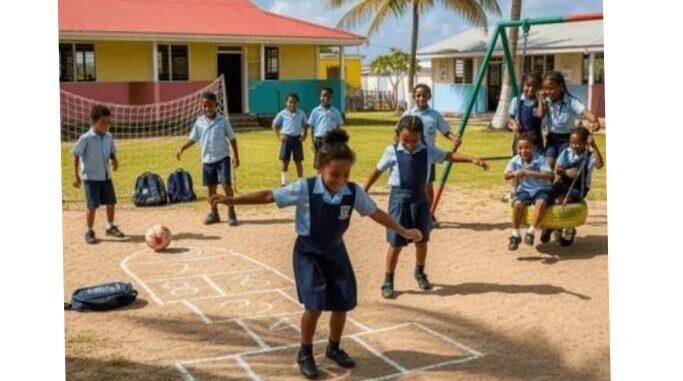
For generations of Caribbean children, the sounds of outdoor play filled open green spaces and paved sidewalks across every island. Shouted calls of “RUN!”, “HOME!” and “OUT!” spurred spontaneous sprints across fields, dodges during competitive games, and mad dashes for safety long before the phrase “physical activity” entered common public discourse. Movement was not a scheduled chore or a gym membership requirement—it was woven into the very fabric of childhood, experienced through the simple, joyful act of play.
Every island across the region nurtured its own unique traditional games that kept bodies moving constantly. In Barbados, children transformed ordinary sidewalks into makeshift road tennis courts, wielding rough wooden paddles to rally back and forth across boundaries marked in chalk. Across Trinidad and Tobago, hopping games like Scotch, Moral and Peesay built coordination and rhythm, while marble matches kept children crouched for hours, steadying their hands to aim and compete. Jamaica’s beloved Dandy Shandy and Stuck and Pull had kids running, laughing, and twisting to break free from grips, filling the air with squeals of delight. Rounders, chase, circle games like “Bluebird In and Out the Window” and “Bull in the Pen” turned empty lots into hubs of constant, unstructured movement, with every community adding its own rules, calls, and shared memories.
Today, however, this rich tradition of spontaneous outdoor play has faded from Caribbean schoolyards and neighborhoods. The rise of screen time, packed modern schedules, and shrinking public play spaces have replaced the shouts of childhood with silence. This shift is far more than a loss of nostalgia: modern public health conversations around physical activity increasingly center on formal gym memberships, structured workout programs, and performance metrics, erasing the deep cultural foundation of free movement that once kept generations healthy.
For decades, unstructured play served as an informal, wildly effective pillar of Caribbean public health. It built physical strength, fine motor coordination, emotional resilience, and tight social bonds across communities without any formal policy or programming. But the decline of childhood movement has left a measurable public health crisis in its wake.
Non-communicable diseases (NCDs) such as hypertension, type 2 diabetes, and heart disease now account for more than 70% of all deaths across the Caribbean, giving the region one of the world’s highest rates of premature NCD-related death among people aged 30 to 70. While poor diet, tobacco use, and excessive alcohol consumption are key contributors, physical inactivity is a major driving force behind the crisis. Today, 30 to 40% of Caribbean adults fail to meet the World Health Organization’s recommended weekly physical activity targets—a trend that traces back to the disappearance of unstructured play in childhood. The “stillness” that settled into schoolyards decades ago now follows people into adulthood, placing enormous strain on regional healthcare systems that bear the cost of long-term chronic disease treatment, medication, and ongoing care.
Current public health prevention efforts often focus almost exclusively on changing adult behavior, rather than restoring the community and school environments that made natural daily movement the norm for generations. Local advocates argue that reviving traditional childhood play is not a trip down memory lane—it is a core public health intervention that recognizes good health is built early in life, through collective community action.
Already, regional policy frameworks reflect this growing understanding. CARICOM member states have formally affirmed the public right to health, and the Caribbean Public Health Agency’s (CARPHA) Six-Point Policy Package targets NCDs and childhood obesity across the region through targeted policy action. Regional campaigns under the umbrella of Caribbean Moves promote active lifestyles, supporting national initiatives including Jamaica Moves, Dominica’s Fit for Life Campaign, St. Lucia’s National Physical Activity Day, and Barbados’ Creative Play Initiative. Countries like Jamaica have also introduced policy measures targeting NCD risk factors, such as a proposed tax on sugar-sweetened beverages, signaling growing recognition of the need to address the root causes of chronic illness.
Advocates emphasize that the next step is not to draft new, unfulfilled commitments—it is to fully implement the promises policymakers have already made. Crucially, this means centering safe, accessible unstructured play as a core public health priority, rather than sidelining it as an afterthought.
As the world marks World Day of Physical Activity and World Health Day, the message from Caribbean public health advocates is clear: movement is not a privileged lifestyle choice, it is a human birthright and a core part of Caribbean cultural heritage worth protecting. To truly prevent chronic illness and build healthier communities, policymakers, schools, and community leaders must make space for the same joyful, traditional childhood play that defined generations—just like the good old days.